................
Return To Main COVID-19 Resource Page
................
Who Is Dr. Byram Bridle?
Current Positions:
• Associate Professor of Viral Immunology – Department of Pathobiology, University of Guelph, Ontario Veterinary College
• Faculty Affiliate – One Health Institute, University of Guelph
Education and Employment Background:
• BSc – Biomedical Science (University of Guelph, Guelph, ON)
• MSc – Immunology (University of Guelph, Guelph, ON)
• PhD – Immunology (University of Guelph, Guelph, ON)
• Postdoctoral fellowship – Oncolytic Immunotherapy (McMaster University, Hamilton, ON)
To learn more about Dr. Bridle, go here.
................
Current News:
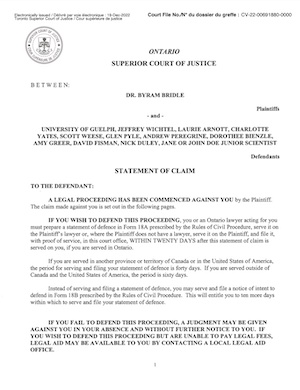
On December 19th, 2022, Dr. Byram Bridle issued a Statement of Claim in Ontario Superior Court. The expert vaccinologist, and viral immunologist, states that he has been viciously and falsely attacked by some of his colleagues, with the complicity of the University administration. Some of the Defendants include the President of University of Guelph, Dean Wichtel, Administrator Arnott, Professor Pyle, Professor Weese, and Dr. David Fisman at the University of Toronto.
Click here for the PDF Statement of Claim
• Crush The Science - Dr Bryam Bridle And The Suppression Of Scientific Debate (Spector World - 10/11/21)
................
Dr. Byram Bridle On Japan's Dangerous, Extremely Concerning, Self-Amplifying RNA Vaccines
................
Steve Kirsch Interviews Dr. Byram Bridle
................
• Stop Masking Children: They Need To Interact With The Microbial World (Byram W. Bridle - 05.31.22)
I want to make parents aware of two harmful aspects of masking children that I am in a position to comment on:
1. Isolating children from the microbial world promotes the development of chronic diseases.
Young children need to interact with the microbial world. It is absolutely essential to the proper development of their immune systems. I am not going to delve into too many scientific details here because I wrote about this in an article that I published in The Conversation in March 2021. It is entitled "A year of COVID-19 lockdown is putting kids at risk of allergies, asthma and autoimmune diseases".
In a nutshell, we are born with naïve and immature immune systems. Our immune systems don't fully mature until well into the teenage years, with most of that development occurring between birth and about six years of age.
The ability of the immune system to self-regulate relies on interactions with the microbial world; especially via interactions with other people, particularly family members. This allows their immune system to learn to differentiate between things that are dangerous and those that are not. In turn, their immune system will become equipped to respond to dangers while preventing potentially harmful responses to things that pose no threat, such as self and inert environmental molecules and normal gut-resident bacteria, etc.
Isolating a young child from non-dangerous microbes in their environment compromises the 'immunoregulatory' components of their immune system. A dysregulated immune system often manifests itself in the form of allergies, asthma, and autoimmune diseases.
I felt compelled to write about this concern in May 2021 after I witnessed children being chronically isolated for more than a year. One year was the timepoint at which I felt that substantial, potentially irreparable harm could be done to children's immune systems. I am appalled that many children have now been enduring this for well over two years, with no end in sight for some.
Masking is controversial and, arguably, largely ineffective against preventing the spread of viruses in ways other than via coughing and sneezing. However, they can pose a reasonable barrier to larger environmental particles (e.g., dust particles, dander, pollen, etc.) and bacteria. Throw in the excessive use of things like antibacterial hand sanitizers, being locked down in homes and lack of physical interactions, and we are now well on our way to having a micro-generation of children who will have been isolated like no other human beings in history. Unfortunately, these children will now be part of an unanticipated experiment on a global scale; one to really assess the validity of the so-called 'hygiene hypothesis'. Although I would like to be wrong on this one, basic immunological principles suggest that very young children that had to endure COVID-19 lockdown policies might be faced with the highest rates of autoimmune diseases, allergies, and asthma in human history.
2. Masking children harms speech development.
I am not a formally trained expert in child development or speech pathology. However, I do have a child who has been dealing with delayed speech development. Through this, I have learned that observing lip, mouth and tongue placement and movements is critical to the proper development of speech. For example, here is a chart known as a 'vowel ladder' that my wife and I use to work with my son to improve his enunciation…
Moving Forward
The moral of this story is to stop isolating our children from their microbial world. Let them get dirty. Let them interact with other children. Let them hug family members and friends. Consider getting a cat or dog that they can interact closely with. Take them on hikes in the woods or countryside. Definitely have them wash their hands with regular soap, but cut down on the antibacterial soaps and sanitizers. Every time normal flora on the skin are killed one risks having them re-populated with pathogens.
And, for goodness sake, let children see the mouths of others so they can learn to speak properly.
What harm is done from the last two-and-a-half years is done. But, please, let’s not keep locking down, physically distancing and masking our children ad nauseum. Not for SARS-CoV-2, not for the annual flu, not for monkeypox. Not for anything unless it is demonstrated via transparent, objective, publicly disclosed and openly debated science to be a genuine threat to the lives of a substantial proportion of children...
................
An Open Letter To The President Of The University Of Guelph (pdf)

................
Dr. Byram Bridle: "The More Vaccinated The Country, The More Problems They Are Having..."
Excerpts:
"The more vaccinated the country, the more problems they are having with COVID-19."
"It is absolutely, 100 percent impossible to achieve the goal of herd immunity with these vaccines."
"What I have seen way too much of and it does cause me very serious concern is that we are seeing people who had cancers that were in remission or that were being well controlled and their cancers have gone completely out of control after getting the vaccine. We do know that the vaccine causes at least a temporary drop in T-Cell numbers. T-Cells are part of our immune system and they are the critical weapons that our immune system has to fight off cancer cells . . . I would say that [this is] my newest major safety concern and it is also the one that is going to be by far the most underreported in the adverse event database. And that's because if a person had a cancer before the vaccine there is no way public health officials will ever link it to the vaccine. But what we are seeing is oncology teams that had pushed the cancers into remission and keeping them well controlled can no longer control them after the vaccine."
"Our system [in Canada] is never going to work. First of all, we're not informing people when they get the vaccine that they are supposed to report any unusual medical condition up to eight weeks after receiving a dose of the vaccine. And the attending physician is required, by law, to report anything unusual, but most physicians are not. Many don't because they don't want to contradict the current narrative and the College of Physicians and Surgeons of Ontario have turned out to be incredibly tyrannical and are crushing many physicians -- and threatening many -- who don't go with this narrow public health narrative. Many also can't get their submissions done because they are onerous. For example, in British Columbia, it can take up to 40 minutes to submit one of these reports . . . And once a physician does submit a report, it doesn't go into our database. It goes to a local medical officer of health . . . and we are seeing unusually high percentages of these reports . . . being rejected at the level of the local medical officer of health . . . Because of all the filtering that is going on, we are not getting accurate numbers."
"More than half the people that have died in this pandemic would be alive today if we had accepted these early treatment strategies [using ivermectin and hydroxychloroquine, for example]. That's the reality. I've seen it with every physician who has administered this. They talk about our ICUs being overrun but every physician that I have worked with -- and I have worked with many -- who have used these effective treatment strategies, they've kept their patients out of the ISU. They don't go to the ISU. They don't die."
"I usually don't ever, ever criticize anybody's expertise in a particular area of work, but we are in unique times. So I think the public needs to be aware . . . The average family physician knows almost nothing about immunology and certainly [almost nothing] about vaccines. Vaccinology is a sub discipline of immunology . . . They are not immunologists. They are not vaccinologists. They are ignoring the vaccinologists."
"People who keep arguing that those of us who have legitimate concerns are wrong, we are providing misinformation, we are lying, we don't know what we are talking about need to ask themselves why then are many of us standing there in the arena, like the gladiators of old, waiting, and none of their champions will step forward . . . I've issued invitations to every single person who attacks me; I invite them to come on and talk publicly . . . I've asked thousands of people and not one person, not even one, in all these months has been willing to talk openly, publicly about the science of medicine underlying COVID-19. It is exceptionally frustrating!"
"The problem of COVID, the number of cases, has been dramatically over-estimated, but to an unknown degree, because of the way we have misused the PCR tests. And we know that the problems associated with the vaccines have been grossly underestimated, also to an unknown degree. Until we have accurate numbers for these -- and I can't see [how] we are going to have anytime soon unless we completely change the way we are monitoring these things -- we're not going to be able to come up with accurate assessments as scientists."
"A bad flu season would be about .1 percent . . . We are actually dealing with a problem that is less fatal than the annual flu, especially when we are talking about children."
................
Rhonda Patrick vs. Byram Bridle - Coronavirus Vaccination (Dryburgh.com - 07/14/21)
................
Dr. Byram Bridle: "We Made A Big Mistake!"
................
MP Sloan, Dr. Bridle, Dr. Phillips: Censorship Of Canadian Doctors & Scientists
................
COVID-19 and Children: A Scientist's Guide for Parents (pdf)
Executive Summary
Pfizer BioNTech’s COVID-19 mRNA vaccine has been Authorized under an Interim Order by Health Canada for use in Canadians as young as 12 years old, with mandatory commitments for the monitoring of long-term safety and efficacy. Authorization under an Interim Order means additional information is needed on the safety, efficacy, and quality of the vaccine, including in children and adolescents, to support the future full market approval and licensing of the vaccine.
There is some uncertainty regarding the long-term safety of Pfizer BioNTech’s COVID-19 vaccine in all individuals, and especially in children, youth, and younger adults of child-bearing age. Indeed, some key safety studies appear to have been missed in the rush to roll out the vaccines, and more is being learned about the vaccines every day. For example, there was a previously wide-held assumption that vaccination with the mRNA vaccines is safe because it is a localized event in the body, with the vaccine remaining limited to the shoulder muscle following injection and triggering an immune response in the local lymph nodes. However, there is evidence that Pfizer’s COVID-19 vaccine does not remain at the injection site. In fact, once injected, the vaccine contents appear to travel extensively throughout the body, to the brain and other sensitive tissues, such as bone marrow, spleen, liver, adrenal glands, ovaries etc. Whether these body sites are involved in producing the spike protein is not known, as this was never studied. Nonetheless, new data have been published that, following vaccination with the Moderna vaccine (an mRNA vaccine very similar to Pfizer’s mRNA vaccine), the spike protein can enter the circulatory system. Presumably, this means the spike protein can travel extensively throughout the body. It is important to understand which organs are producing the spike protein, what factors result in the spike protein entering the circulation, how long the spike protein circulates, and in which body fluids (e.g., semen, saliva, breast milk, urine) the spike protein is present. This information is incredibly important because recent data have come to light that the spike protein is “biologically active”. This means that the spike protein is not just an antigen that is recognized by the immune system as being foreign. It means that the spike protein, itself, can interact with receptors throughout the body, called ACE2 receptors, potentially causing undesirable effects such as damage to the heart and cardiovascular system, blood clots, bleeding, and neurological effects. Although some might argue that the risk of the spike protein causing this type of damage is only a theoretical risk, when we are mass vaccinating a population of predominantly healthy people, including children, adolescents, and adults of child-bearing age, there is absolutely no room for avoidable error.
The current scientific uncertainties demand that the administration of Pfizer’s COVID-19 vaccine to children, adolescents, and young adults of child-bearing age be paused until proper scientific studies that focus on the safety and pharmacokinetics and biodistribution of the vaccines and the vaccineencoded spike protein can be conducted.
Halting the vaccination can be done safely because:
• The risk of severe and potentially lethal COVID-19 in these specific populations is so low that we need to be very certain that risks associated with mass vaccination are not higher;
• Asymptomatic members of this population are not a substantial risk for passing COVID-19 to others; and Page 3 of 37
• There are effective early-treatment strategies for the very few children, adolescents, and young adults of child-bearing age who may be at risk of developing severe COVID-19, such as ivermectin, fluvoxamine, and budesonide. It is not appropriate to use an “experimental” vaccine in a population group unless the benefit of vaccination exceeds the risk of vaccination in that population group. With risk of severe COVID-19 in children, adolescents, and young adults of child-bearing age already so low, the benefit of vaccinating these population groups with a vaccine for which neither the long-term safety nor efficacy is known cannot be concluded to exceed the risk. In other words, the risk of serious COVID-19 is so low in children, adolescents, and young adults of child-bearing age that the standards for safety must be set much higher for them...
COVID-19 and Children: A Scientist's Guide for Parents (pdf)
................
Do Masks Work? Viral Immunologist Dr. Byram Bridle Performs A Simple Experiment To See...
................
Return To Main COVID-19 Resource Page
................